
In many ways, coronavirus has functioned like an x-ray. With the flip of a switch, it has stripped us of our skin and revealed our internal state, which was once so deliberately hidden, so to avoid the gaze and judgment of the outside world. We are left exposed, vulnerable, illuminated.
In this state, we are confronted with a new awareness: our world as we choose to perceive it does not necessarily match the truth of how it functions. The racism that so many people believe to have been buried in our history long ago now clearly presents itself in the racial demographic data—or lack thereof—for COVID-19. The classism that has divided our society into the haves and have-nots is now revealed with deadly implications, as access to testing or treatment depends on one’s connections and ability to pay, respectively. Numerous other forms of inequality and injustice are becoming apparent, as I will argue throughout this piece—each of which provides further evidence to the point that coronavirus is an x-ray that has quite tragically revealed just how broken our bones are.
When coronavirus first spread through Wuhan, so too did the x-ray’s exposure: illuminating a pervasive fear of the other, and the xenophobia that follows; exposing how we speak before we think, and the extent to which we project our own prejudice. According to press reports, on February 2, an Asian American woman in Chinatown was attacked for wearing a face mask; and on March 10, another Asian American woman was attacked for not wearing a face mask. It seems you’re damned if you do, and you’re damned if you don’t. Consider these stories without the mention of any face mask: two Asian American women were attacked. Our x-ray confirms what it’s like to be a minority in this country. What it’s like to be a woman.
This is what coronavirus looked like when it was “theirs” and not “ours.” But the virus finally did the inevitable and spread to our soil. And so too did the unforgiving gaze of that which strips skin, tears tissue and loosens ligaments. The resultant x-ray image displayed the ease with which we sacrifice our own, as if we had already collectively decided which lives were worth saving—and which were not.
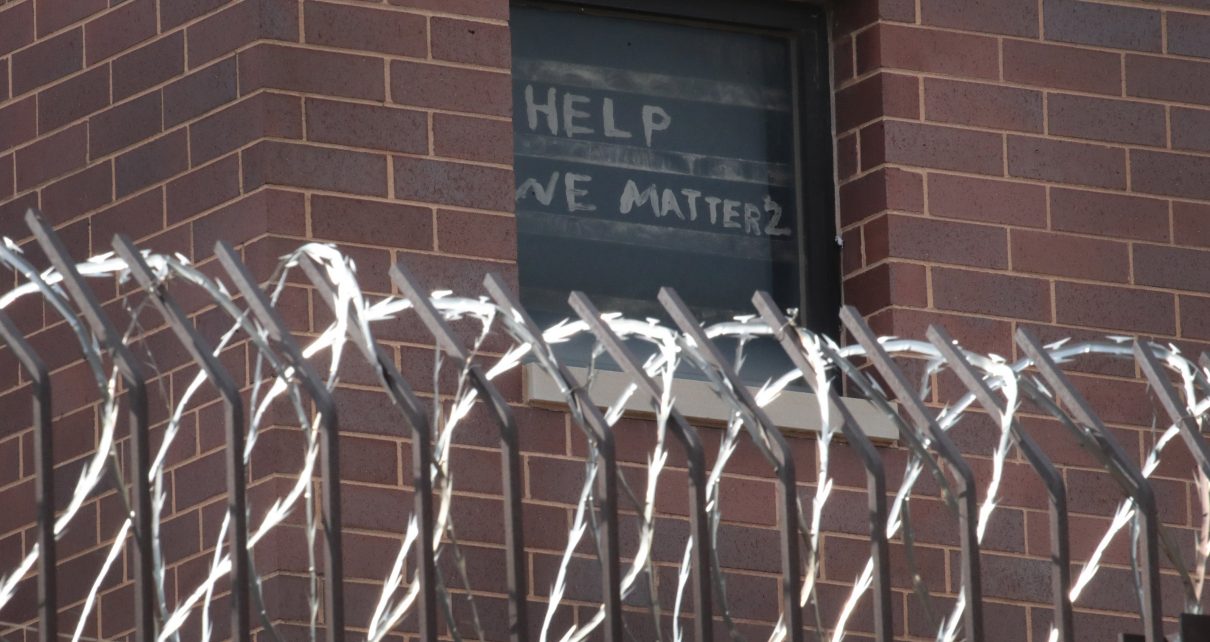
I read a headline on April 20: “73% of Inmates At An Ohio Prison Test Positive For Coronavirus.” Now why is that unsurprising? America’s inmates are some of our most vulnerable people, and they are also some of our least protected. Should we not offer our most protection to our most vulnerable? We do so with children—coddling them with safety precautions and protective measures, so they feel a bit more empowered. A little less vulnerable. Now think about situations of mismatch: where an individual’s relative vulnerability is not mirrored in her relative level of protection. Do you have individuals in mind? Perhaps entire communities? And how are they faring with the pandemic?
Because the prison population is but one example. A community that is overcrowded—in Ohio, specifically, filling nearly 130 percent of intended capacity—insufficiently protected and hence suffering disproportionately. There have been marginal efforts to alleviate this problem, by freeing some inmates, but the efforts themselves are problematic. For one, the numbers released are small, and often even these have sparked political resistance. And I cannot help but wonder, whom do authorities choose to release and why? Because if the release process in any way reflects the incarceration process, something tells me it may not be fair. If white inmates are more readily released than inmates of color, are we not exacerbating the racial disparities in our criminal justice system? Indeed, at the federal level, an algorithm that the Justice Department is relying on for such decisions has raised fears it will produce racially biased results.
In general, data about race and COVID-19 are insufficient. The Trump administration has announced that it will not disclose the details of how the disease is affecting different racial groups until early May—raising the question of whether this delay is being used to gather the most factual and comprehensive data possible, or if instead the delay is obscuring what we already know to be true: minorities, specifically black persons, in our society have time and time again been disproportionately negatively affected during emergency situations or crises. We need not look beyond 2005, when Hurricane Katrina ravaged the same area of New Orleans that is now facing an astonishing COVID-19 infection rate of 1,637.4 per 100,000 people. But if we did, and we jumped back in time to 1927 Mississippi, we would note that of the victims of the state’s Great Flood, 90 percent were black.
Now, we are seeing similar trends, but on a much larger scale. As of April 3, black Americans represented 81 percent of COVID deaths in Milwaukee, despite only making up 26 percent of the population in that area. At that same point in time, 70 percent of Chicago’s deaths from COVID-19 were black Americans, who make up only 29 percent of the city’s population. Similarly, in Michigan, black persons in early April represented 40 percent of COVID-19 related deaths—more than three times their share of the population.
And black Americans are not the only minority group being disproportionately affected. As of mid-April, COVID-19 infection and hospitalization rates among Latinos in Utah were three times those of the state’s white population; and there, as well as in Oregon, New Jersey and Washington— three other states that had released demographic data—the proportion of Latino COVID-19 patients was nearly double that of Latino residents.
Moreover, even the racial and ethnic data that exists are incomplete. There has been at least one instance of a Latino COVID-19 victim’s body being incorrectly identified and recorded as “white” when deceased. Such mistakes would have the dual effect of decreasing the number of counted Latino deaths and increasing the number of counted white deaths—thus reducing the perceived ethnic disparity. And Trump’s hostility to undocumented Latino immigrants had already made such individuals more fearful about seeking health care. In consequence, such immigrants may be less likely to get tested for COVID-19, again tainting the demographic data.
The pandemic has made it abundantly clear that the well-connected and well-to-do enjoy a degree of privilege that directly benefits their own COVID-specific health outcomes and those of surrounding people, who are presumably from a comparable socioeconomic background. Celebrities and other social elites have been able to be tested for COVID-19 even if they are asymptomatic, when such options have not been readily available to the average person.
If one of these wealthier individuals were to test positive, they would likely have enough square footage in their house to self-quarantine in a relatively comfortable fashion and not put their family members at risk of infection. Furthermore, if they were to develop severe systems, they would also probably have a health insurance plan that would cover their treatment. Now to contrast this situation with individuals who are less socioeconomically stable; they are more likely to live in crowded homes where self-quarantining may not even be possible, not have an insurance plan to cover the costs of COVID-19 care, or might even depend so much on a regular paycheck that they still need to attend work while sick—thus exposing other persons to the virus.
These issues, however, are not the faults of poorer persons, just as they are not the faults of minority groups, or of the incarcerated. The issues are instead rooted in the structural injustices that gave rise to disparities on the basis of wealth, race, ethnicity and criminal status. Perhaps now more than ever before, we can see those structural injustices—illuminated, exposed, revealed. They are, in fact, difficult to ignore.
This, I argue, is the x-ray effect. The coronavirus has spread across the world like a dark substance—blinding us with fear, arresting us in uncertainty. But once we flip that switch, that is, once we ignite the radiation, we are made aware of what exists beneath the surface: all that our aesthetic world has strategically covered up or ignored. And with that awareness comes the responsibility to attend to the issues that have been previously neglected and the persons who have been historically burdened. The examples I offered above are only a few that have come to light since the beginning of our global pandemic. We are also witnessing prejudice against elderly populations, persons with disabilities, rural communities, homeless persons and other vulnerable groups.
So just as an earthquake is bound to first destroy the structures that are least sound, and a hurricane will swallow anything already struggling to stay afloat, a pandemic disproportionately takes the lives already compromised. They are our society’s most vulnerable, and our least protected; not for who they are, but for the meaning and sense of worth that our systems have projected onto them. So, the systems are the problem. And the systems are our bones. The skeletal system of our society, which we expect to support us—not to betray us. But upon closer look, from our pandemic perspective, our bones are broken.
No, shattered.

